
Mallet finger is a condition where the end of the finger is bent and does not straighten. It occurs when the extensor tendon on the back of the finger is damaged. The finger joint is a hinge-joint that allows bending and straightening of the fingers. Each finger is composed of 3 phalanges (finger bones), joined by 2 interphalangeal joints (IP joints). The joint near the base of the finger is called the proximal IP joint or PIP joint, and the joint near the tip of the finger is called the distal IP joint or DIP joint.
Mallet finger occurs from sports activities causing a “jammed” finger or from excessive stress on the finger such as with a crushing injury. The injury causes either rupture of the extensor tendon without a bone fracture or rupture with a small or large bone fracture.
Generally, mallet finger can be treated non-surgically using specially designed splints that immobilise the finger and promote natural healing. In cases of fracture, complete bone healing may take 8-12 weeks, followed by physiotherapy for strengthening. In severe cases that don’t respond to conservative treatment, surgery is recommended.
If left untreated, mallet finger can develop into a finger joint deformity referred to as a swan neck deformity.
Causes
Mallet finger occurs due to sports activities (such as baseball) or other activities that cause a direct and forceful impact on the fingers.
Signs and Symptoms
The main symptoms of mallet finger are drooping of the finger at the distal joint, pain and swelling around the area and limited range of motion at the joint.



Diagnosis
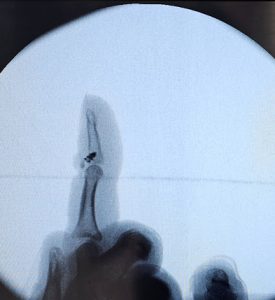
The diagnosis of mallet finger involves a physical examination and obtaining an X-ray of the injured finger. In some cases, other imaging techniques such as MRI scan may be recommended.
Treatment
Mallet finger can be treated non-surgically by applying a specially designed splint for 8-12 weeks. Immobilising the finger with a splint helps promote natural healing of the torn tendon or bones. Dr Bala prefers a malleable aluminium splint applied onto the back of the finger fixing the joint in a little bit of extension with non-stretch tape.





For patients who require use of their fingers to perform occupational tasks, internal splints can be used; this involves surgical placement of metal pins in the affected bones. The pins can be removed after 6 weeks of healing.



Patients who fail to achieve adequate relief may be recommended for surgery which involves repairing the torn tendon. If the mallet finger involves a fracture of the bone fragment, then it can be stabilised and fixed using pins or very small screws.

If the tendon has pulled off with a very small piece of bone or without bone then the tendon can be reattached with a suture anchor (which is a metallic screw with attached sutures) or a special hook plate. A wire maybe placed across the joint for 3 weeks if it is unstable.


In chronic untreated injuries Dr Bala may advise fusion of the fingertip joint to improve function and cosmesis. This is done through the back surface of the finger just above the nail. The cartilage of the joint is removed and bone graft from the back of the wrist is put into the joint. The joint is stabilised in the neutral position with a headless titanium screw under x-ray guidance. An aluminium splint is applied for 4- 6 weeks after surgery to aid fusion of the joint.

Post-operative care
After mallet finger surgery, the patient is recommended for physiotherapy for flexibility and strengthening exercises.
Risks and complications
The common risks and complications associated with mallet finger surgery, include:
- Avascular necrosis (bone death from lack of blood supply)
- Infection
- Stiffness
- Nail-bed damage
- Chronic tenderness
- Skin necrosis

Untreated mallet finger can lead to a swan neck deformity

Dr Bala uses special magnification loupes to visualize and protect individual blood vessels and nerves in this region to minimize complications.